
Treating Pulsatile Tinnitus Associated With Sigmoid Sinus Wall Anomalies
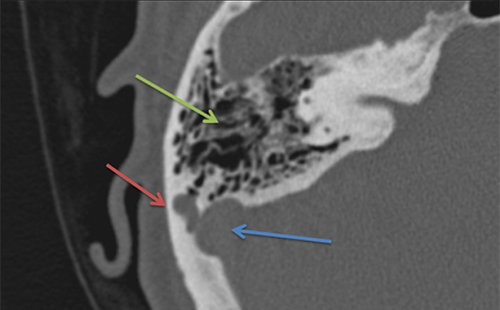
Axial CT of right temporal bone – The red arrow indicates lobulated sigmoid sinus diverticulum, the blue arrow indicates sigmoid sinus, and the green arrow indicates mastoid air cells.
A surgeon at the University of Maryland Medical Center (UMMC) discovered a solution to cure a common cause of pulsatile tinnitus (PT) with a 95% success rate.
In a recent study, David J. Eisenman, MD, Associate Professor of Otorhinolaryngology - Head and Neck Surgery at the University of Maryland School of Medicine and Director of Otology and Neurotology at UMMC, discovered a strong association between sigmoid sinus wall anomalies (SSWA) and transverse sinus stenosis (TSS). The findings suggest that TSS, which is highly prevalent in patients with SSWA, plays a role in the production of PT in these patients. It also suggests a connection between SSWA and idiopathic intracranial hypertension (IIH), a problem known to be associated with PT.
By discovering new clinical and radiographic features of sigmoid sinus wall anomalies and their association with PT, Eisenman was able to completely resolve PT in thirty-six out of 40 subjects (90%) through a modification of a conventional mastoidectomy approach.
Since the study was published in 2018, Eisenman has diagnosed and successfully treated an additional 36 patients from all over the country with PT with his procedure, taking the success rate to 95%.
In addition to discovering the clinical importance of sigmoid sinus diverticulum and dehiscence as causes of PT, Eisenman also found that women of childbearing age with an elevated body mass index (BMI) are commonly affected. He also found that there is a high rate of empty sella in these patients, another finding strongly associated with IIJ.
While transtemporal sinus wall reconstruction generally has a high success rate in appropriately selected patients, patients with isolated sinus wall dehiscence without diverticulum, TSS, or empty sella are less likely to respond to transtemporal sinus wall reconstruction. This data implies a multifactorial cause of PT in at least some patients with SSWA.