
Managing CSF Leaks with Titanium: An Effective, Patient-Focused Approach
Cerebrospinal fluid (CSF) surrounds and cushions the brain and spinal cord to protect these delicate organs. Spontaneous fluid leaks occur when there is a hole or tear in the dura mater, at times causing fluid to drain through the nose (rhinorrhea) or the ear (otorrhea).
CSF leaks can also result in headache, infection (meningitis), tinnitus (ringing in the ears), or visual problems. They are more likely to occur in middle-aged women with elevated body mass index (BMI) and in those with a history of idiopathic intracranial hypertension (IIH, high CSF fluid pressure).
A 2021 study showed that participants with CSF leaks had a mean age of 60, which was significantly greater than those with IIH or sigmoid sinus wall anomalies (SSWA). Patients with CSF leaks also demonstrated a higher rate of hypertension, which increases intracranial pressure (ICP). This suggests that age-related factors may contribute to CSF leaks and that elevated ICP likely needs to be chronic, causing greater skull defects, for a CSF leak to occur.
University of Maryland Medical Center (UMMC) employs a patient-focused and customized approach to repairing CSF leaks. A multidisciplinary skull base team, typically including specialists from neurosurgery, neuroradiology, and otolaryngology (neurotology and rhinology), provides treatment.
The reparation approach used depends on the location of the leak and the size and location of the skull base defect, but commonly involves surgery. Surgical materials also vary. Both rigid and soft tissue elements may be employed.
When titanium mesh is the deemed the most appropriate material, UMMC leverages an advanced approach as a bone graft substitute for successful repair of the middle cranial fossa skull base.
Shown to be safe and effective, titanium mesh provides the rigidity of a bone graft without donor site morbidity and increased operative time. It is also easily contoured and rigidly fixed in place, unlike bone grafts that may migrate and protrude into the cranial vault.
Studies show that the risk of infection with titanium is not considered higher than other synthetic materials used for reconstruction (bone cement, fibrin glue, silastic sheets). It also demonstrates a low rate of graft infection (2.6%) compared with alternatives such as autogenous bone grafts (25.9%).
How is Titanium Used?
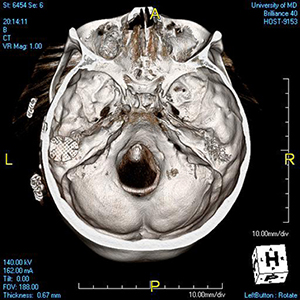
First, an orbital floor titanium mesh reconstruction plate is cut to an appropriate size and shape to reconstruct the bony defect in the floor of the middle fossa. This allows the flanges to extend through the floor of the craniotomy and be secured in the zygomatic root and bony buttress of the superior mastoid cortex.
Next, a soft tissue graft is placed to cover the floor of the middle fossa. The titanium mesh plate is reinserted and secured with screws. A second layer of soft tissue graft is then inserted between the plate and dura, and the entire reconstruction is covered with synthetic fiber sealant.
Finally, the bone flap is replaced and secured, the wound is closed in layers, and a pressure dressing is applied.
UMMC finds titanium mesh plates immediately prevent CSF leaks and symptom recurrence with no postoperative side effects.
For more information or to refer a patient for evaluation or treatment to the Department of Otorhinolaryngology-Head & Neck Surgery at UMMC, please contact 1-800-373-4111.
References
- Bhatnagar K, Patel L, Gourishetti S, Raghavan P, Eisenman DJ. Imaging Characteristics of Sigmoid Sinus Wall Anomalies, Idiopathic Intracranial Hypertension, and Spontaneous CSF Leaks. Otol Neurotol. 2021;42(6):945-951.
- Khan A, Lapin A, Eisenman DJ. Use of titanium mesh for middle cranial fossa skull base reconstruction. J Neurol Surg B Skull Base. 2014;75(2):104-109.